
A Tradesman Who Had Never Needed a Chiropractor
This 48-year-old HVAC technician had gone his entire life without chiropractic care. He was physically capable, active in his trade, and carried the assumption that many working men carry: if something hurts, rest it, and it will recover. That approach had served him well enough — until it didn’t. He picked up a piece of heavy equipment, felt something go wrong in his low back, and was unable to return to work. The severity of the situation forced him to seek care for the first time.
He came in expecting to address one problem in one location. That is not how the spine works, and the X-ray examination confirmed it. His lumbar spine was significantly subluxated, which was expected. What emerged during care was not.
What We Found — and What Emerged During Care
Clinical Findings — Initial & Developing Presentation
Patient: 48-year-old male HVAC technician
Mechanism: Acute injury lifting heavy equipment; no prior chiropractic history
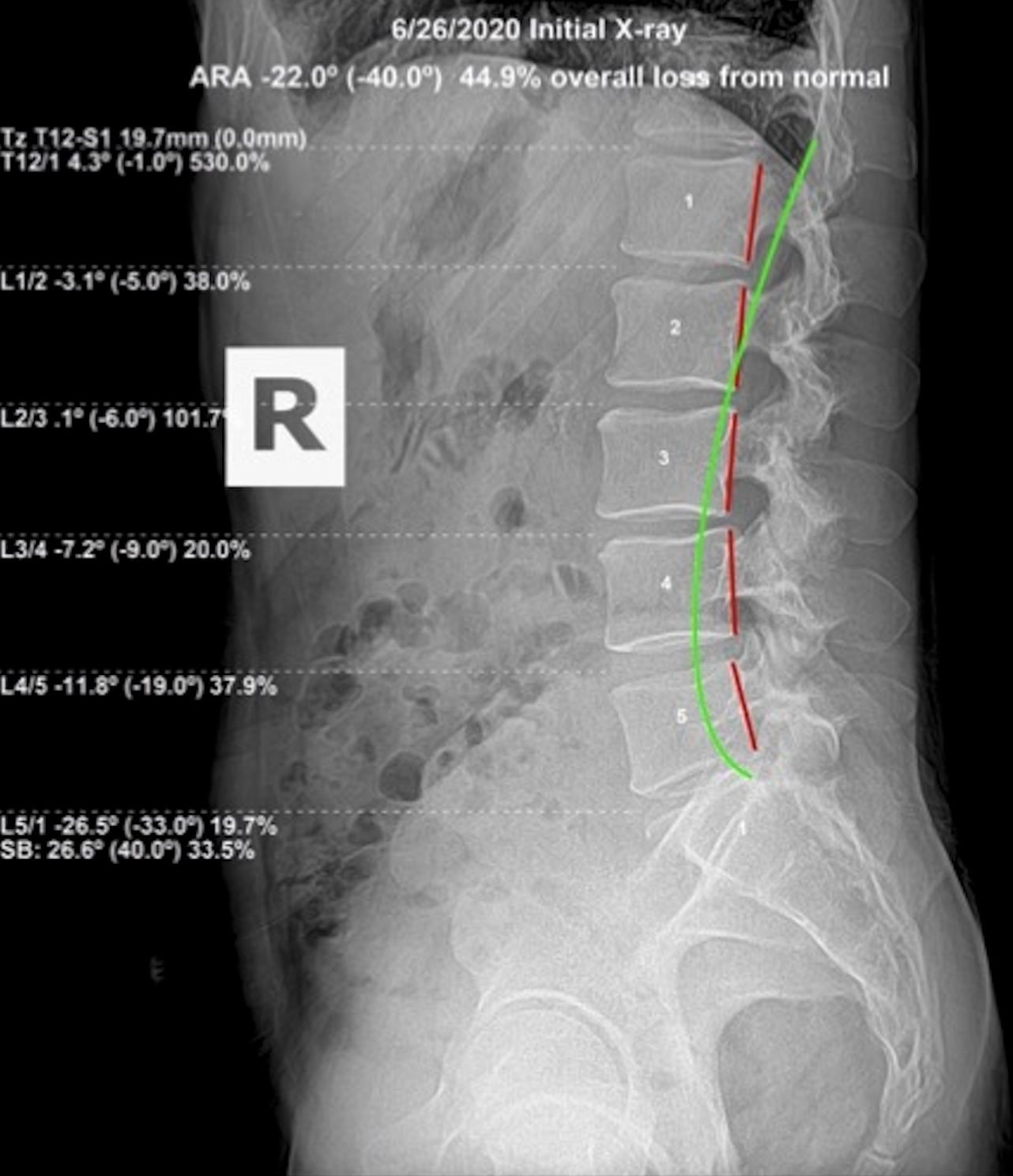
X-ray type: Lateral lumbar
Initial ARA: −22.0° (normal −40.0°) — 44.9% overall loss from normal
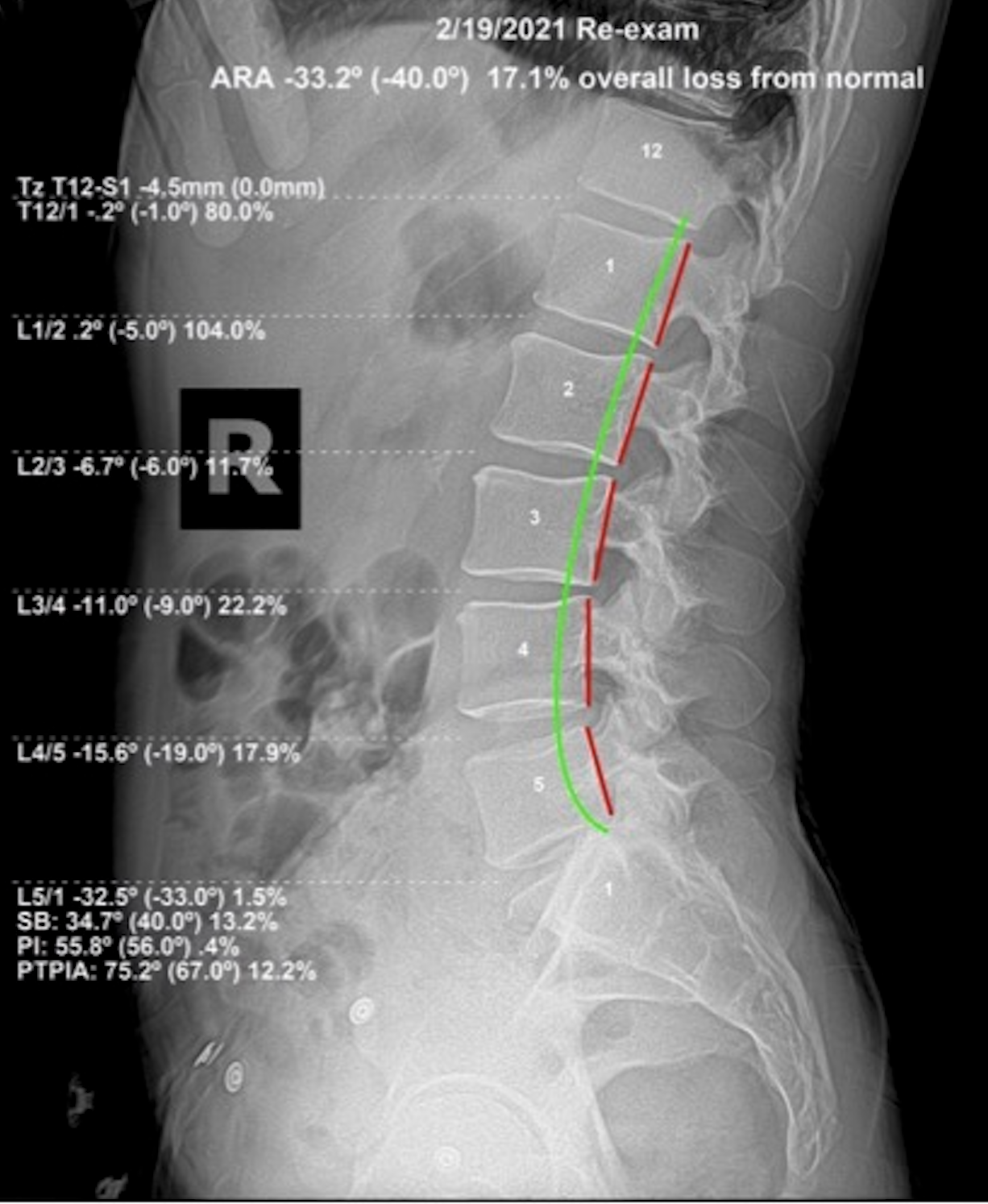
Re-evaluation ARA: −33.2° (normal −40.0°) — 17.1% overall loss from normal
Emerging finding: Cervical subluxation became symptomatic during lumbar correction process
Supplemental: McKenzie disc therapy for lumbar disc restoration
Duration: Approximately 6 months of corrective care
As his corrective adjustments began — addressing the full spine, not only the lumbar region — his cervical spine started producing more discomfort than his low back. He had never noticed his neck before. That is common. Cervical subluxation can be present for years without producing symptoms that the patient associates with the neck. When the lumbar spine began to be corrected, the compensation patterns that had masked the cervical subluxation were disrupted, and the neck made itself known.
This is also when the lumbar correction became more complex. Straightening the lumbar curve in isolation — when the cervical spine above it is also subluxated — places compensatory stress on the entire column. We incorporated McKenzie disc therapy to restore disc position in the lumbar region, which supported the structural correction work. We also spent considerable time in education: explaining to him how the cervical and lumbar regions are part of one mechanical system, and why addressing both was necessary to produce lasting results.
Lumbar Lateral — Before & After
He Stayed the Course — and the Results Were Self-Evident
After conversations about the whole-spine nature of his subluxation complex and how the cervical spine influences lumbar mechanics, he made the decision to stay with the full corrective protocol. Approximately six months later, the results were, as the newsletter stated, self-evident. His ARA measurement moved from −22.0° (44.9% loss from normal) to −33.2° (17.1% loss from normal) — a dramatic structural improvement documented on lateral lumbar film.
There is a principle in this work that is worth stating plainly: spinal correction is not linear. The body retraces, the nervous system reorganizes, and what feels like setbacks in the early weeks is often the system adjusting to the structural changes being made. The results are reproducible when the principles of subluxation correction are applied consistently and when the patient trusts the process long enough for the X-ray to confirm what the body is already expressing. He returned to work. He returned to function. He did so without surgery.
Why This Pattern Matters
The work injury case reveals something important about how the spine adapts to cumulative stress. This tradesman had been performing physical labor for years — carrying, lifting, working in confined spaces, twisting under load. His lumbar curve had been compromised long before the lifting incident that brought him in. That single event did not create the subluxation. It was the moment that finally exceeded the body's capacity to compensate.
Physical tradespeople present this pattern with regularity. They carry the assumption that their bodies can handle more because they always have. What they don't account for is that each year of accumulated mechanical stress narrows the margin. The final event feels like the cause. The X-ray shows it was the last straw.
The other significant finding here — that correcting the lumbar spine revealed cervical subluxation that had been masked — is a reminder that the spine is one connected structure. Correcting one region changes the mechanical load distribution throughout the whole. What appeared to be a low back problem required full spinal correction. That is subluxation-based structural chiropractic working as it should.
There is also a clinical distinction in how this injury was addressed that separates the outcome from what a standard medical pathway would have produced. A work injury presenting with acute low back pain and significant loss of lumbar lordosis would typically enter a treatment pathway focused on pain management, anti-inflammatories, and physical therapy. Those interventions do not change the ARA measurement. They do not restore lumbar lordosis. They relieve symptoms while the structural deficit that caused the injury remains in place. This patient's ARA moved from 44.9% loss to 17.1% loss — that is structural change documented on film. No medication or physical therapy produces that result.
The decision to stay with the full corrective protocol — including the cervical work that emerged mid-plan — reflects a patient who chose to address the whole structural reality rather than just recover enough to return to work. That decision changed the trajectory. Workers who complete corrective care at this level are not just returning to their previous state. They are returning to a structurally sounder foundation than they had before the injury occurred.
The cervical finding that emerged after the lumbar correction was underway illustrates a structural pattern that full spinal evaluation is designed to capture from the outset. When the lumbar spine begins to correct and the compensation it had been maintaining through the thoracic and cervical regions starts to shift, secondary subluxation that was masked by the primary lumbar pattern becomes visible — both on X-ray and in how the patient responds to care. Full spinal correction requires the follow-through to address what the clearing of the primary problem reveals.
The combination of lumbar and cervical correction changes the patient's structural trajectory in a way that lumbar correction alone would not. The cervical spine governs brainstem function; the lumbar spine governs pelvic stability and lower extremity neurological supply. Correcting both produces a nervous system that is decompressed at two major levels simultaneously. The occupational capacity outcomes this patient experienced were the result of both corrections working together — not either one in isolation.
What to Look For
For anyone who performs physical labor — trades, construction, landscaping, athletic training — the early signs of developing lumbar subluxation tend to be dismissed as part of the job. Stiffness after a long day that used to resolve overnight but now takes longer. A preference for one side when lifting. Recurring lower back tightness after specific movements. These are compensatory patterns, not simply muscle fatigue.
The important signal is when recovery time lengthens. If something that used to clear in a day now takes three, the body's compensatory capacity is narrowing. The acute incident that stops a tradesman in his tracks is rarely the beginning of the problem. It is the end of the body's ability to work around a subluxation that has already been present for some time.
A structural evaluation before that incident — not after it — is the better choice.
For workers in physically demanding trades, the structural evaluation after a significant injury is not a one-time event. The spine that was compensating before the injury will continue to accumulate load after it. Periodic structural check-ins — with a lateral X-ray and ARA measurement — provide an objective baseline that tracks structural health over time. The patient who corrects through a significant occupational injury now has a structural baseline that any future incident can be measured against. That is a different kind of occupational health protection than workers' compensation alone provides. Have you ever had your spine checked for subluxation?
A Work Injury Is a Spinal Event. Address It at the Spine.
If you have injured your back lifting, twisting, or performing physical labor, the pain you feel is a signal about your spine — not just a muscle problem. A structural X-ray evaluation will show what is actually happening and give us a clear corrective target. Do not manage it. Correct it.
Schedule a Structural EvaluationOr call us at (561) 795-3156