How She Arrived — and What She Was Carrying
This 53-year-old woman came to Rochet Family Chiropractic referred by a patient who had been with us for years. That is how much of our best care happens — one person who has experienced structural correction firsthand, who sees someone they care about struggling, and who says: go see Dr. Rochet. She arrived with a presentation that had no mystery to it. Severe low back pain. Radiating pain into both legs. Weakness. Pins and needles. The signs commonly associated with sciatic nerve involvement. She described it as a “hot low back.” She could not stand fully upright. She could not exercise. She could not walk to the corner and back with her friends. Another case of “I don’t know what happened. I didn’t do anything.”
The story is familiar because the pattern is familiar. Vertebral subluxation does not announce itself with a single event in most cases. It accumulates over years of uncorrected structural stress, until the nervous system can no longer compensate and the signals become impossible to ignore. When she arrived, her lumbar spine and pelvis were significantly subluxated. The job was to correct those structures and let Innate Intelligence do the rest.
What We Found and How We Worked
Clinical Findings — Initial Examination
Patient: 53-year-old female, referred by long-time practice member
Presenting complaints: Severe low back pain, radiating leg pain, weakness, pins and needles, inability to stand straight or exercise
X-ray type: AP lumbar and pelvis
Primary subluxation region: Lumbar spine and pelvis
Adjustment distribution: Lumbar adjustments 20–25% of visits; majority of adjustments delivered to pelvis
Supplemental therapy: McKenzie disc therapy to restore disc position
Time to initial improvement: Within one week of initiating care
Her care plan involved specific chiropractic adjustments to the lumbar spine and, predominantly, to the pelvis — which is the structural foundation of the entire lumbar column. When the pelvis is subluxated, the vertebrae above it compensate, and the nerve roots exiting the lumbar spine are placed under stress. Correcting pelvic subluxation removes that foundational mechanical interference first. We also performed McKenzie disc therapy to encourage the discs of her lumbar spine back toward their normal position, which supports the holding capacity of the surrounding vertebral corrections.
Lumbar & Pelvic AP — Before & After
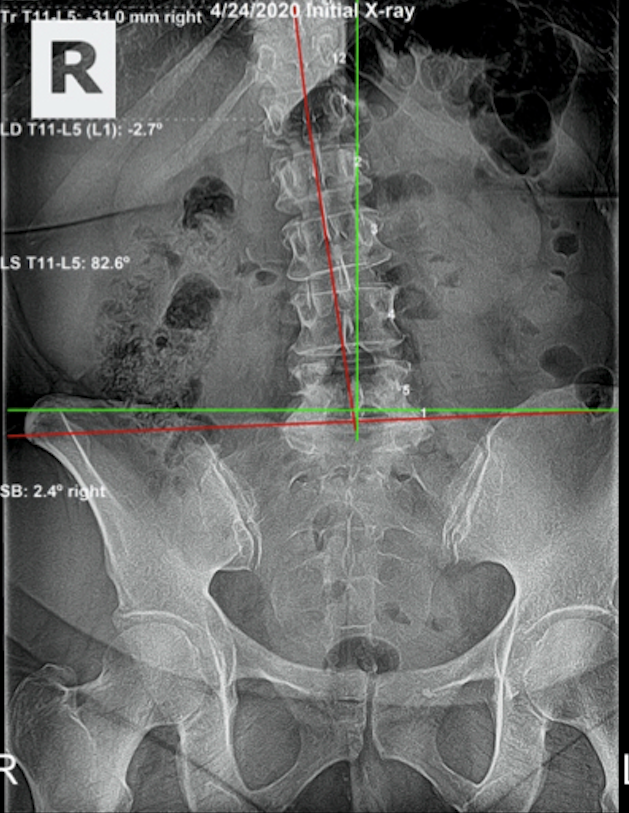
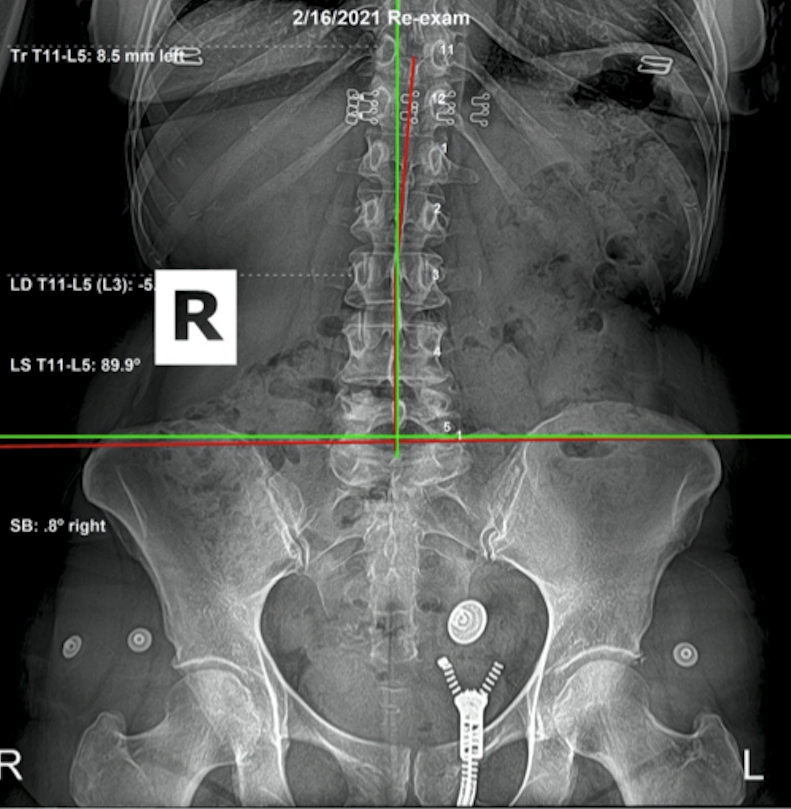
What the X-Rays Confirmed — and What They Cannot Show
The follow-up X-ray taken February 16, 2021 confirmed significant improvement in both lumbar and pelvic alignment. That is visible, measurable, and objective. What the X-ray cannot show — but what matters just as much — is the quality of life that returned with the structural correction. She took approximately one cumulative month off during her care plan, and the results still speak for themselves.
Her quality of life upon completing the initial corrective plan was higher than it had been before she ever started experiencing these difficulties. Her activities of daily living were not merely restored — they were more satisfying than before. That is what Innate Intelligence, operating through a structurally corrected spine, is capable of. I move the bone. God does the healing. The body is designed to express life, and it does so most fully when the nervous system is free of interference.
Why This Pattern Matters
The pelvic foundation is the structural base of the entire lumbar column. When the pelvis is subluxated, every vertebra above it compensates. The lumbar vertebrae stack on an unlevel base. The discs absorb asymmetric load. The nerve roots exiting the lower lumbar and sacral spine — the pathways that become the sciatic nerve — are placed under mechanical stress at the most fundamental level. The pelvis has to be corrected first.
This is why the adjustment distribution in her case was skewed heavily toward the pelvis, even though the lumbar spine was where she experienced the problem most intensely. Structural correction follows what the X-ray shows, not where the patient hurts. That principle is what separates subluxation-based care from symptom management.
She came in unable to walk to the corner. Within one week of pelvic and lumbar correction, her nervous system had enough structural room to begin the process her Innate Intelligence had been working toward the entire time. By the end of the plan, her quality of life exceeded what it had been before the difficulties began. That is not unusual. That is what the body is designed to do when the interference is removed.
This case also demonstrates what the referral relationship means in a principled practice. The patient who referred her had experienced her own structural restoration. She recognized the pattern in her friend's situation — the disability, the inability to walk, the dependence on others — and made the connection to what correction had done for her. That is how structural chiropractic spreads through a community: through people who have experienced the outcome and can identify the same structural picture in someone they care about. The referral was an act of knowledge, not sales.
One month of cumulative missed appointments during a corrective plan is also worth noting. It did not prevent the structural correction. It likely extended the timeline. Corrective care is not all-or-nothing — but consistency matters. The body needs repeated, precise correction applied at appropriate intervals to hold and deepen structural change. The results in this case, despite the interruptions, confirm that committed structural correction produces documented outcomes even when real life introduces gaps.
The referral origin of this case also contains structural information about patient readiness. A patient who arrives because a close friend described their own structural correction arrives with prior knowledge — what the X-rays showed, what the adjustment process involved, what changed in the friend's body. That background eliminates the educational gap that most new patients start with. The referred patient already understands that the goal is structural change verified by comparative X-ray. They are aligned with the corrective model before the first visit.
The missed appointments in this case also document something clinically important: even incomplete corrective care within a specific structural plan can produce meaningful results. This should not be read as permission to skip visits. It is an observation about the spine's structural responsiveness when the adjustments that are delivered are specific and correctly sequenced. The improvement documented on the re-evaluation film was achieved despite a portion of the prescribed visits being missed. Full attendance would have produced more complete correction in the same window.
What to Look For
Pelvic and lumbar subluxation tend to accumulate silently. The first signs are often postural: one hip higher than the other when standing; a tendency to shift weight to one side; uneven shoe wear. The low back may be stiff in the morning and gradually loosen through the day — a sign that structural stress is present but the body is compensating through movement.
Radiating leg pain — numbness, tingling, or weakness traveling into the buttock, thigh, calf, or foot — is a sign that the subluxation has progressed to active nerve root involvement. At that stage, structural evaluation is urgent. The longer nerve roots carry that level of interference, the longer the resolution takes. Early correction, before the neurological signs appear, is always more straightforward than correction after they do.
When the disability is acute — inability to walk normally, extreme pain with any weight bearing, dependence on others for daily activities — it can be tempting to seek immediate pain management as the first response. That is understandable. But pain management does not address the structural source. The case documented here shows that aggressive structural correction, begun even at the acute stage, can produce functional return within days. The structural investigation belongs at the beginning, not as a last resort. Have you ever had your spine checked for subluxation?
Radiating Leg Pain Is a Structural Problem. Treat It Structurally.
If you are experiencing low back pain that travels into your legs, weakness, tingling, or inability to stand or walk normally, your spine needs a structural evaluation — not pain management. Come in for an X-ray analysis and let us find out what is actually happening in your lumbar spine and pelvis.
Schedule a Structural EvaluationOr call us at (561) 795-3156