A Debilitating Back Injury and a Fear That Went Deeper Than Pain
This 66-year-old man was referred to Rochet Family Chiropractic by a fellow practice member who had experienced remarkable results through subluxation correction. He arrived with a presentation that was immediately serious: severe back pain radiating into both legs, weakness, and pain so significant that he could not drive himself to the appointment. He had suffered a debilitating injury that compounded an already stressed spine.
Imaging revealed the full picture. There was age-related degeneration. There was spondylosis. There were disc changes. The medical recommendation was surgery. But his greatest fear was not the surgery itself — it was what surgery would require him to stop doing. He was an athlete. He skied. He lifted weights. Surgery, in his mind, meant the end of that identity. The practice member who referred him had seen similar fears dissolve through chiropractic correction. He wanted to find out for himself.
What the X-Rays Showed — and What Five Months Produced
Clinical Findings — Lateral Lumbar X-Ray Analysis
Patient: 66-year-old male athlete, referred by practice member
Presenting: Severe bilateral radiating leg pain, weakness, unable to drive; spondylosis, disc degeneration
X-ray type: Lateral lumbar
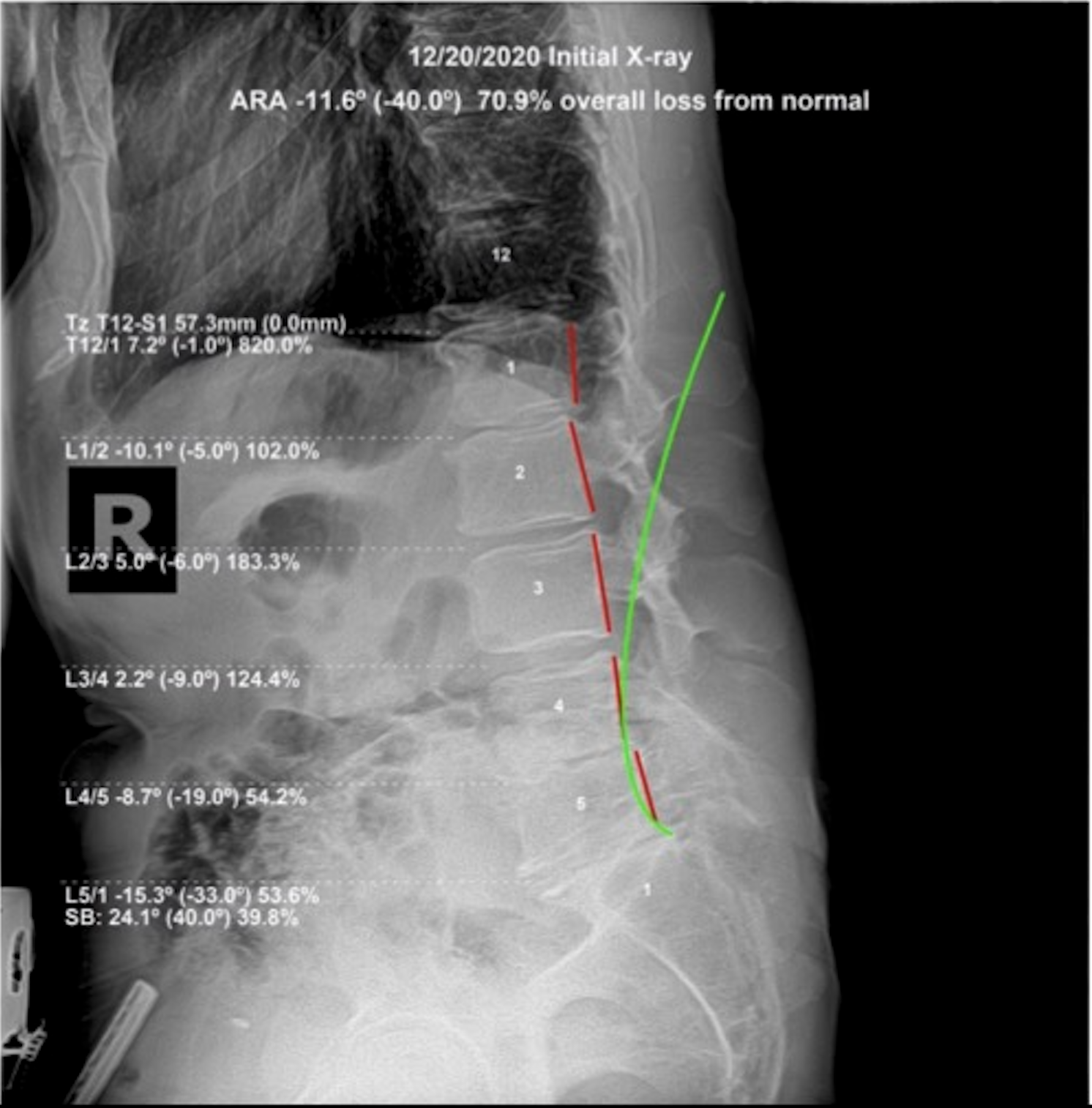
Initial ARA: −11.6° (normal −40.0°) — 70.9% overall loss from normal
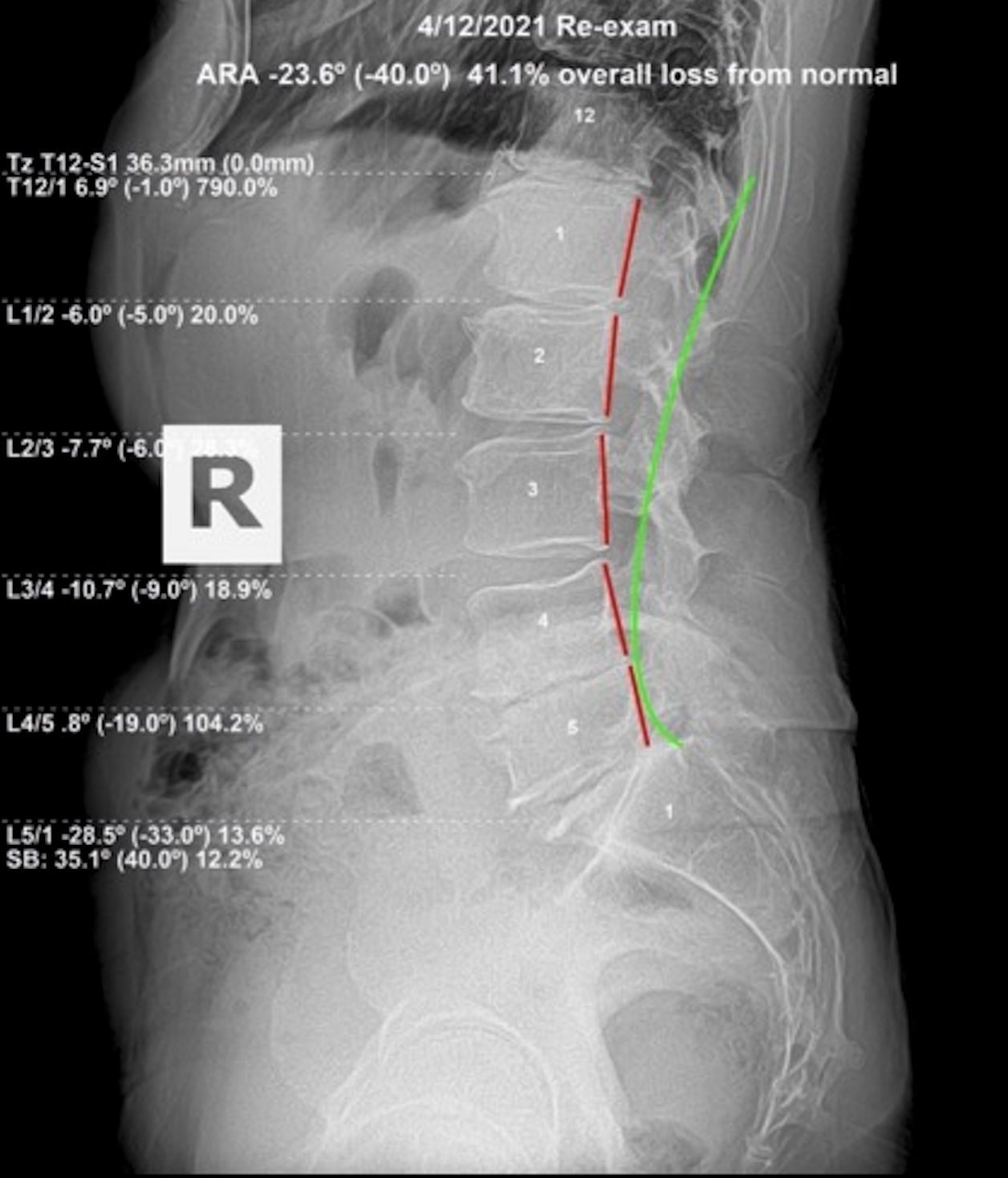
Re-evaluation ARA: −23.6° (normal −40.0°) — 41.1% overall loss from normal
Duration: Approximately 5 months of subluxation-focused corrective adjustments
Outcome: Full return to ADLs; surgery no longer under consideration; higher QOL than before injury
His initial lateral lumbar X-ray showed a lumbar ARA of −11.6 degrees against a normal of −40 degrees — a 70.9 percent overall loss from normal. This is a severely reduced lumbar lordosis, meaning the natural curve of the low back had been largely lost. When this curve collapses, the mechanical load on the lumbar discs and vertebrae increases dramatically, accelerating degeneration and compressing nerve root pathways. It was a structural problem producing structural consequences, and it required a structural correction.
Lumbar Lateral — Before & After
The Fear That Went Away — and the Life That Returned
After approximately five months of subluxation-focused corrective spinal adjustments, the re-evaluation lateral lumbar X-ray showed his ARA had improved to −23.6 degrees — a 41.1 percent loss from normal. That is a measurable, documented structural change in a 66-year-old spine with spondylosis and disc degeneration. The body is designed to heal when the interference is removed. That is not a marketing claim. That is what these X-rays confirm.
More importantly: he returned to his full activities of daily living. Surgery was no longer being considered. His biggest fear — losing the ability to ski, to lift weights, to be an athlete — had dissolved. He was experiencing a higher quality of life than he had before the injury. That is what Innate Intelligence, operating through a structurally corrected spine, is capable of producing — even at 66, even with degeneration, even when surgery was on the table. I move the bone. God does the healing.
Why This Pattern Matters
The athlete case challenges an assumption embedded in how spinal degeneration is typically explained to patients: that once degeneration is present, the trajectory is fixed. Surgery is framed as intervention; everything else as management. This case says something different.
Degeneration is a consequence of sustained mechanical stress. The structural source of that stress — the subluxation — is correctable. When the subluxation is addressed and the mechanical environment of the spine improves, the body has a better foundation to work with. The degeneration itself doesn't disappear. But the ongoing insult that accelerates it is removed, and the remaining healthy tissue gets the conditions it needs to function.
What moved this patient's ARA from −11.6° to −23.6° was specific subluxation correction in a 66-year-old spine with documented spondylosis. That is a 29.8-percentage-point improvement in lumbar lordosis, achieved without surgery. It returned him to skiing and weight training. Innate Intelligence does not stop working because of age or degeneration. It works with what exists. Subluxation correction gives it better conditions to do so.
What also deserves attention is the fear dimension of this case. He was referred by a fellow practice member who had experienced remarkable outcomes. He came in with degeneration, disc involvement, and a surgical recommendation. The fear of losing his athletic identity was real. That fear was resolved not by managing pain but by restoring the structural integrity that allowed the body to function. When the spine is corrected and Innate Intelligence is operating without structural obstruction, the body does not merely reduce pain — it recovers capacity. This is the clinical claim that X-ray documentation makes credible.
Age is also not the limiting factor this case is often assumed to represent. The spine of a 66-year-old with spondylosis and disc degeneration does not have the same correction potential as a 25-year-old's — but it has more than most people, and most physicians, expect. The measurement tells the truth. The ARA improved. The patient returned to function. That happened at 66 with structural degeneration present. The ceiling for what structural correction can achieve in an older spine is consistently underestimated.
This case also documents something about the role of age in structural correction that is frequently misrepresented to older patients. Sixty-six years old, documented spondylosis, disc degeneration, a lumbar ARA 29.8 percentage points below normal — and the correction produced a 29.8 percentage-point ARA improvement. The body's structural responsiveness at 66 is not a function of age alone. It is a function of how much correctable subluxation is present and how consistently it is addressed. The degeneration was not reversed. The subluxation was. Innate Intelligence used the remaining healthy tissue to express the correction the structural conditions allowed.
The surgical recommendation this patient received was not made with the benefit of a subluxation-specific structural assessment. The imaging showed degeneration. The recommendation followed the imaging. What the imaging could not show was whether the structural source of the symptoms included a correctable subluxation underlying the degenerative picture. In this case, it did. The degeneration remained. The subluxation was corrected. The symptoms resolved and the patient returned to skiing and weight training. Age was not the limiting factor. The evaluation that preceded surgery was the limiting factor — until it was replaced by one that was.
What to Look For
In older patients and in anyone with a long history of physical activity, the early signs of significant lumbar subluxation with disc involvement are often described as stiffness rather than pain. Getting up from a chair takes a moment. The lumbar spine doesn't flex forward as easily as it used to. Standing upright after prolonged sitting requires a few steps before it normalizes.
When radiating leg pain begins — even mildly — the nerve roots are already involved. That is not the beginning of the process; it is the point where the subluxation's effect has extended beyond the joint. At that stage, a structural X-ray evaluation matters: it tells you how much lumbar lordosis remains, how the discs are presenting, and whether there is a correctable subluxation underneath the degenerative picture. Degeneration plus subluxation is a different clinical reality than degeneration alone. The subluxation is the variable that can be changed.
If a surgical recommendation has been made based on imaging that shows degeneration, the structural evaluation for subluxation has likely not been completed. Degeneration on MRI is not a surgical indication on its own. The question is whether the mechanical environment producing the symptoms includes a correctable subluxation. In many cases, it does. A structural X-ray evaluation before agreeing to surgery is always worth pursuing. Have you ever had your spine checked for subluxation?
Degeneration Is Not a Death Sentence. Subluxation Is the Variable We Can Change.
If you have been told your spine is degenerating and surgery is the answer, get a second opinion — from your X-ray. Structural correction does not reverse degeneration, but it restores the mechanical environment that allows your body to function at its full potential within that degeneration. Come in for a structural evaluation and find out what is actually correctable.
Schedule a Structural EvaluationOr call us at (561) 795-3156