A Complex Case With Legitimate Complications
This 24-year-old woman presented at Rochet Family Chiropractic with a history that most chiropractors would approach with caution — and rightfully so. Prior to seeking our care, she had undergone multiple surgeries on her legs and hips to correct congenital structural deformities. These surgeries are not minor events for the spine. Surgery always alters spinal biomechanics. The structural relationships that the spine depends on for its normal load distribution and corrective holding capacity are changed permanently when hardware is introduced, joint mechanics are modified, or soft tissue is cut and repaired.
This is one of the most important things I communicate to patients in complex cases: our expectations for spinal correction are always high, but complicating circumstances always play a factor. We do not lower our standards. We calibrate our expectations honestly, pursue the best possible result through specific subluxation correction, and let Innate Intelligence determine what the body can achieve within its structural reality. Then the X-ray tells us what actually happened.
Nine Months — and What the X-Ray Showed
Clinical Findings — AP Lumbar X-Ray Analysis
Patient: 24-year-old female
Complicating history: Multiple prior surgeries on legs and hips for congenital structural deformities
X-ray type: AP lumbar
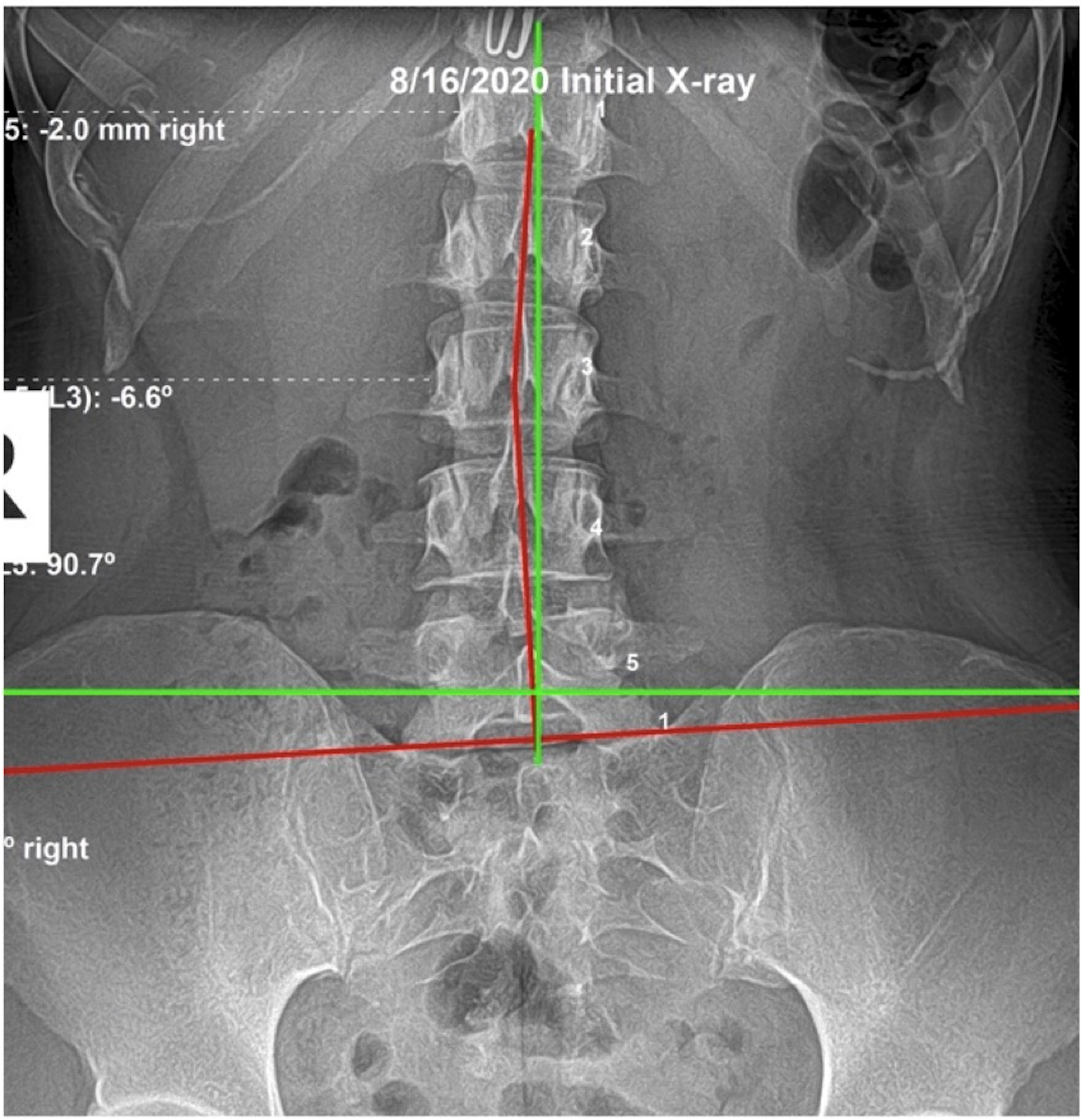
Initial X-ray: Aug 10, 2020 — significant lumbar subluxation with altered mechanics from surgical history
Duration of care: 9 months
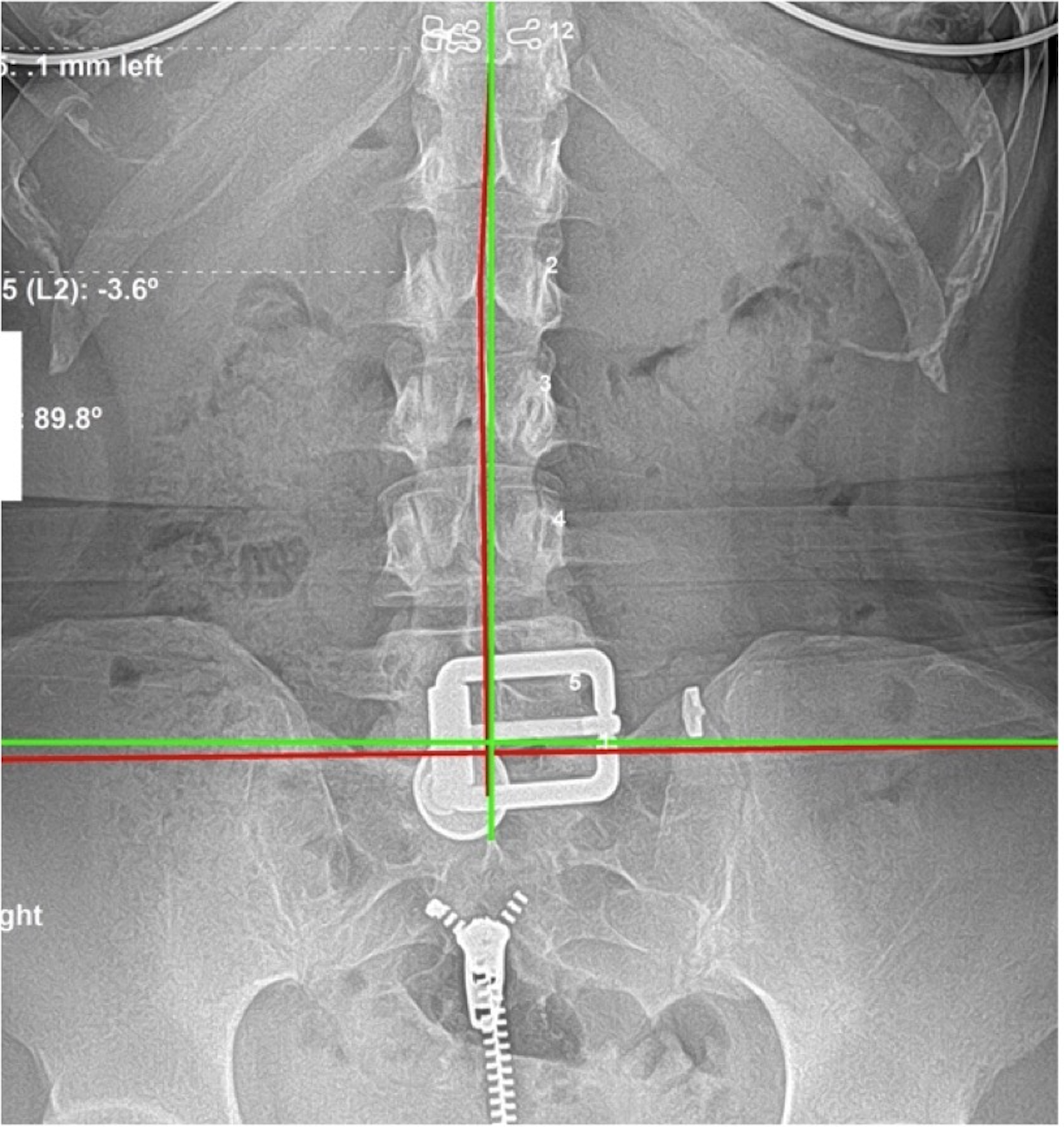
Re-evaluation result: Near-perfect spinal correction on AP lumbar film
QOL outcomes: Significant improvement; increased ADLs; resolution of original symptoms
She was under care for nine months — longer than a standard corrective plan, reflecting the complexity of her case and the need for more time to produce meaningful structural change in a post-surgical spine. The AP lumbar X-ray findings at the outset showed the expected pattern: significant subluxation in a lumbar region whose mechanical environment had been altered by the surgical history below. The correction process was deliberate, consistent, and patient.
Lumbar AP — Before & After
What Near-Perfect Looks Like — and What It Means
The re-evaluation AP lumbar X-ray is the record. As the newsletter stated: her spine went through a near-perfect correction. That result — in a 24-year-old with multiple prior surgeries and congenital structural deformity — is exceptional. It reflects what the body is designed to do when the interference is removed and Innate Intelligence is allowed to operate through a spine that has been structurally corrected to the best degree possible.
Her quality of life outcomes were, if anything, equally as significant as the X-ray. She increased her activities of daily living in ways that mattered to her. The original symptoms that brought her into care resolved. The surgical history that we expected to limit her correction did not stop the body from expressing the health it was created to express. I move the bone. God does the healing. This case is evidence of exactly that.
Why This Pattern Matters
Prior surgery is the most common reason people exclude themselves from pursuing structural correction. The logic seems reasonable: hardware is present, the mechanics have been altered, there is nothing left to correct. What this case shows is that Innate Intelligence doesn't stop working at a surgical scar. The body's capacity for self-correction continues to operate within whatever structural environment exists. The goal isn't to undo surgery. The goal is to correct the subluxation that is present in the spine as it is now.
Post-surgical spines accumulate subluxation in a predictable pattern. When hardware is introduced below or adjacent to a region, the segments above begin bearing altered loads and compensating. The lumbar vertebrae that carry no hardware are still capable of subluxating — and correcting. Near-perfect structural correction in a post-surgical spine doesn't happen because surgery was reversed. It happens because the nervous system, given the structural freedom it was designed to have, expressed the health it was always trying to express. That is Innate Intelligence. No surgery changes what it is trying to do.
The congenital element raises an additional point. This patient had likely been told, implicitly or explicitly, that her structural situation was fixed. Congenital conditions define the starting position, not the end point. The spine she had — with its surgical and congenital history — still reached near-perfect correction on the re-evaluation film. The X-ray measured what actually happened in her body, not what was expected based on her history. Expectations set by prior providers are not clinical measurements.
Nine months of corrective care in this context reflects appropriate scope. A post-surgical, congenitally complex spine requires more time and more precise adjustment sequencing than a structurally simpler presentation. The correction process had to navigate altered load patterns and a nervous system that had been adapting to structural deviation its entire life. The outcome — near-perfect correction on film, full ADL restoration, original symptoms resolved — demonstrates that the body's capacity for structural restoration is not accurately predicted by the severity of the history that preceded care.
The post-surgical spine also creates an expectation problem for patients. Nine months of care feels longer than a standard corrective timeline. But the standard timeline applies to a standard structural presentation. A spine that is navigating congenital deviation, surgical hardware, and decades of compensatory load requires a different — and longer — timeline. The outcome in this case proves the timeline was appropriate. Nine months of correctly sequenced, hardware-aware correction produced near-perfect structural restoration in a spine that had every structural reason to correct incompletely.
The patient's history of being told what her spine was not capable of — implicitly through years of management-focused care — is also a recurring pattern in complex structural cases. Management care communicates a ceiling. Corrective care does not accept that ceiling as permanent. The objective measure in both approaches is the X-ray. The management approach did not produce measurable structural change. The corrective approach produced near-perfect correction on film. The difference between those two outcomes is the goal of care, not the structural complexity of the spine.
What to Look For
After orthopedic surgery to the hips, legs, or lower lumbar region, the spine above the surgical site compensates. Asymmetric low back tension, one hip that sits consistently higher than the other, a persistent sense of imbalance that the surgery itself didn't resolve — these are signs the spine is carrying subluxation load, not evidence the surgery failed. The segments above the hardware remain correctable.
The sooner subluxation is addressed post-surgically, the less compensatory load accumulates in the regions above. Waiting compounds the mechanical problem. If you've had orthopedic surgery and assumed chiropractic care is off the table, get an evaluation anyway. The X-ray shows what is actually there — not what you assumed.
For patients who had surgery years ago and assumed the resulting outcome was permanent — persistent discomfort, restricted mobility, one-sided compensation — the relevant question is whether the subluxation pattern that developed around and above the surgical site has ever been specifically evaluated. Surgery solves what it was designed to solve. It does not prevent subluxation from developing in the segments adjacent to and above the hardware. Those segments are still subject to the structural demands of daily life and still respond to specific correction.
The most important step is requesting a structural evaluation that includes X-ray analysis of the unsurgical regions — not a range-of-motion assessment, not a palpation examination, not an MRI focused on the surgical site. A full spinal X-ray series that measures ARA and identifies subluxation above the hardware tells you what is correctable in the spine you have now, not the spine you had before surgery. That is the evaluation this patient did not have until years after her procedure. When she had it, the result showed a correctable picture. The correction followed. Have you ever had your spine checked for subluxation?
Prior Surgery Is Not a Reason to Stop Pursuing Structural Correction.
If you have had orthopedic surgery and been told chiropractic care cannot help, or if you have assumed your surgical history makes structural correction impossible, come in for an evaluation. Every spine deserves an honest assessment of what is possible. Yours may surprise you.
Schedule a Structural EvaluationOr call us at (561) 795-3156