
Most people who search for this term are really asking a more specific question: is what I have actually fixable? The answer depends entirely on what's causing the problem. If it's subluxation — yes. Here's what that means.
Vertebral subluxation is a misalignment of one or more spinal bones that creates interference in the nervous system — disrupting communication between the brain and the body through the affected nerve pathways. In subluxation-based chiropractic, it is detected through X-ray analysis and neurological assessment, then corrected with a specific adjustment targeted to the exact vertebra, direction, and degree of misalignment. The goal is restored nerve function, not symptom management.
You'll find the word "subluxation" in both medical and chiropractic literature, but with different meanings. In orthopedic medicine it means a partial dislocation: bones partly out of alignment but still in contact. In subluxation-based chiropractic, the word means something more precise — a vertebral misalignment that creates a specific neurological consequence: interference with the nerve signals traveling between the brain and the body.
That interference is what we're looking for. And it doesn't always come with pain.
Your spine houses your most important communication system
And subluxation disrupts it
Your nervous system runs everything. The brain generates signals that travel down through the spinal cord and exit through nerve roots — one pair at each spinal level — reaching every organ, muscle, gland, and tissue in the body. This two-way communication loop governs heart rate, digestion, immune function, hormonal regulation, and more. God designed the body with an extraordinary ability to self-regulate and self-heal through this system.
The spine — 24 movable vertebrae — is the structural housing for that communication. When it's in proper alignment, signals flow. When a vertebra moves out of position and creates pressure on the nerve root at that level, the signal is compromised. That's subluxation.
Lantz CA. "The vertebral subluxation complex." Chiropractic Research Journal. 1989;1(3):23–36.
Here's what most people don't know: only about 10% of your nerve fibers are sensory — meaning they transmit pain. The other 90% govern organ function, immune response, muscle control, and your body's God-given ability to regulate itself. Subluxation can be interfering with all of that long before pain appears. The interference is already happening. The pain comes later, if it comes at all.
A spine that isn't hurting can still be a spine that isn't functioning. That's why we don't rely on symptoms to make care decisions — we rely on analysis.
Where subluxation occurs
Every region, different consequences
Subluxation can happen at any level of the spine, and where it is matters, because each region has different nerve pathways and different consequences when those pathways are compromised.
The neck — most mobile, most vulnerable. C1 (atlas) sits directly beneath the brainstem. Subluxation here can affect brainstem output, autonomic regulation, and nerve pathways throughout the entire body. Full cervical subluxation guide →
The mid-back. Nerve roots here serve the heart, lungs, digestive organs, and intercostal muscles. Thoracic subluxation is common in patients with prolonged forward-flexed posture.
The lower back. Lumbar nerve roots supply the legs, lower abdominal organs, and bladder. L4–L5 and L5–S1 are among the most frequent subluxation sites due to the mechanical demands of the lumbopelvic region.
The foundation of the spine. Sacroiliac subluxation affects pelvic alignment and creates compensatory stress throughout the entire column above. Pelvic subluxation is a common finding in patients with lower extremity imbalance.
The uppermost cervical vertebra — and the most neurologically significant subluxation site. The atlas surrounds the brainstem. Correction here has systemic effects that extend far beyond the neck. It is assessed at every initial examination.
Subluxation rarely exists in isolation. Compensation patterns develop — one misaligned segment creates mechanical stress that causes adjacent levels to shift. Whole-spine analysis is required to find the primary versus compensatory subluxations.
How subluxation is detected
We don't guess. We look.
In our office, we don't adjust until we've seen the spine on film. X-ray is the primary detection tool — specifically, the lateral and AP (front-to-back) views that reveal what symptom history alone never can. Three things in particular:
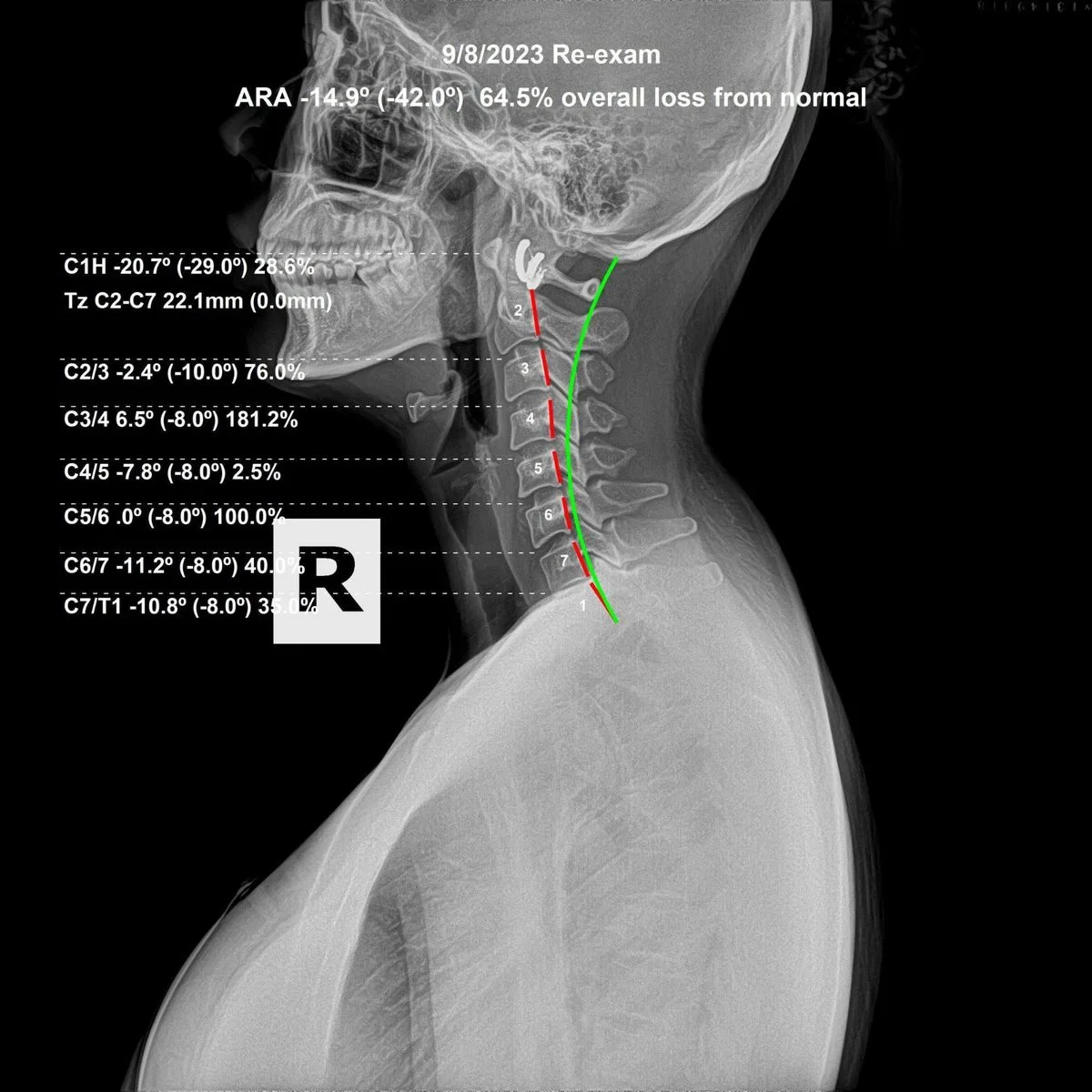
Vertebral position. Each bone's relationship to the ones above and below it — shifted forward, rotated, tilted — is visible and measurable. The direction and degree of misalignment tell us exactly where to adjust and how.
Curve integrity. A healthy spine has natural curves. Chronic subluxation erodes them over time. Curve loss is one of the most reliable structural markers of long-standing subluxation — and a clear indicator of how much correction work remains.
Disc condition. Disc narrowing on X-ray tells us where sustained subluxation has been loading the spine improperly. The disc doesn't narrow overnight — this is years of abnormal mechanical stress made visible.
Spinal X-ray analysis at Rochet Family Chiropractic. Vertebral position, curve integrity, and disc spaces are all evaluated before care begins. Dr. Rochet, Royal Palm Beach FL.
Neurological assessment at every visit, not just the first
After the initial X-ray, we reassess neurological indicators at each visit to determine whether an adjustment is indicated that day — and where. Leg-length checks, postural analysis, specific nerve function tests. We do this every time because the spine is dynamic. The adjustment that was right last visit may not be right today. We follow what the nervous system is showing us — not a preset protocol.
What correction looks like
Specific, not general
A subluxation correction is not general spinal manipulation. It is a specific adjustment — a precise force applied to a specific vertebra, in a specific direction, at a specific angle — based on what the X-ray and neurological findings show at that visit. The goal is to restore the bone to its normal position and remove the interference from the nervous system.
Correction is a process, not a single event. The spine has typically been in the subluxated position for months or years before the first adjustment is delivered. Everything around it — muscle, ligament, connective tissue — has adapted to the misaligned position. That doesn't reverse in one visit. Consistent, progressive care is required. And we document it: follow-up X-rays taken after a period of care show whether the structural changes match the clinical goals.
I've been doing this for 19 years. The look on a patient's face when they see their before-and-after films side by side — when the curve is measurably restored and the vertebrae are back where they belong — that never gets old. That's the difference between adjusting to feel better and adjusting to actually correct something.
Who gets subluxated, and when it starts
Earlier than most people assume
The spine is subject to physical stress from the moment of birth. The birth process produces measurable compressive and torsional forces on the cervical spine — particularly at the atlas. Falls during early childhood, sports impacts, screen posture, desk work, motor vehicle accidents, and the cumulative load of gravity applied over years all contribute to subluxation development at every stage of life.
Subluxation is not a condition of age or injury history. It is found in infants and children, in pregnant patients, in athletes, and in adults with no history of trauma who have simply accumulated postural and mechanical stress over time. It does not self-correct. Subluxations that are not addressed tend to compound — structural changes that begin as positional misalignment progress over years into measurable disc narrowing, curve loss, and degenerative joint change visible on X-ray.
The spine does not self-correct. It accumulates. What starts as a positional problem becomes a structural one — and what starts as a structural problem becomes a degenerative one, visible on X-ray and measurable over time. Don't wait for pain to tell you something is wrong. By then, you're already behind.
Subluxation-based vs. symptom-based chiropractic
The distinction that defines the practice
Not all chiropractors practice the same way. Most chiropractic in the United States is crisis care — the patient comes in when something hurts, gets adjusted until it stops hurting, and leaves. The structural state of the spine is not the concern. Relief is.
That's a different thing entirely. We don't adjust to manage symptoms. We adjust to correct vertebral subluxations. When the interference is removed, the Innate Intelligence of the body — your God-given capacity to heal and regulate — does what it was designed to do. It doesn't need our help to heal. It needs the interference out of the way.
We require X-rays before beginning care. We reassess neurological indicators at every visit. We take follow-up films to verify that the correction is actually occurring — not just that the patient feels better. Not all chiropractic is the same — and the difference is not minor.