Cervical subluxation is a misalignment of one or more vertebrae in the cervical spine — the seven bones of the neck (C1 through C7) — that creates interference in the nervous system. The misalignment disrupts communication between the brain and body through the affected nerve pathways. In subluxation-based chiropractic, it is detected through X-ray analysis and corrected with a specific adjustment targeted to the exact vertebra, direction, and degree of misalignment.
Most people searching for a definition of cervical subluxation just want a straight answer, so here it is: a cervical subluxation is a bone in your neck that has moved out of its normal position in a way that is interfering with your nervous system. That interference matters, whether or not it is causing you pain right now.
What follows is the clinical version — what that actually means, how I find it, and what it looks like when it is corrected.
The cervical spine: seven vertebrae, one critical region
Anatomy and vulnerability
Your cervical spine runs from the base of your skull down to the top of your mid-back. Seven vertebrae, C1 through C7, and the most mobile part of the spine. That mobility has a cost: it is also the most vulnerable to subluxation from physical stress, poor posture, trauma, and the everyday load of life.
C1 through C7 at a glance
Sits at the base of the skull. Surrounds the brainstem. Subluxation here affects brainstem function, blood pressure regulation, and nerve pathways throughout the entire body.
The pivot point for head rotation. The atlas rotates around C2. Subluxation at C2 frequently co-occurs with atlas subluxation and affects the same high-level nerve pathways.
Mid-cervical levels. Nerve roots at these levels serve the diaphragm, shoulders, and upper arms. Subluxation can affect breathing mechanics and upper-extremity function.
Lower cervical levels. Serve the biceps, wrists, and forearms. Among the most common subluxation sites due to cervical curve stress and forward head posture.
The cervicothoracic junction. Nerve roots here serve the triceps and hands. Subluxation at this level is associated with arm and hand numbness.
A normal cervical spine has a lordotic (forward) curve of approximately 40–45°. Loss of this curve — seen on X-ray — is one of the primary structural indicators of chronic subluxation.
How cervical subluxation is detected
What the X-ray shows
I do not assume a cervical subluxation from your symptoms. I find it through analysis. The main tool is the lateral cervical X-ray, and it shows me three things:
The position of each vertebra relative to the ones above and below it. A subluxated vertebra shows misalignment in one or more planes — forward, backward, rotated, or tilted — away from the normal structural relationship.
The cervical curve. A healthy neck has a forward (lordotic) curve. Chronic subluxation, especially up high, makes that curve reduce, straighten, or in advanced cases reverse. It is visible on the film and measurable over time.
The disc spaces. Subluxation puts abnormal mechanical stress on the discs. Narrowed disc spaces on the X-ray show me where sustained subluxation has been loading the spine the wrong way.
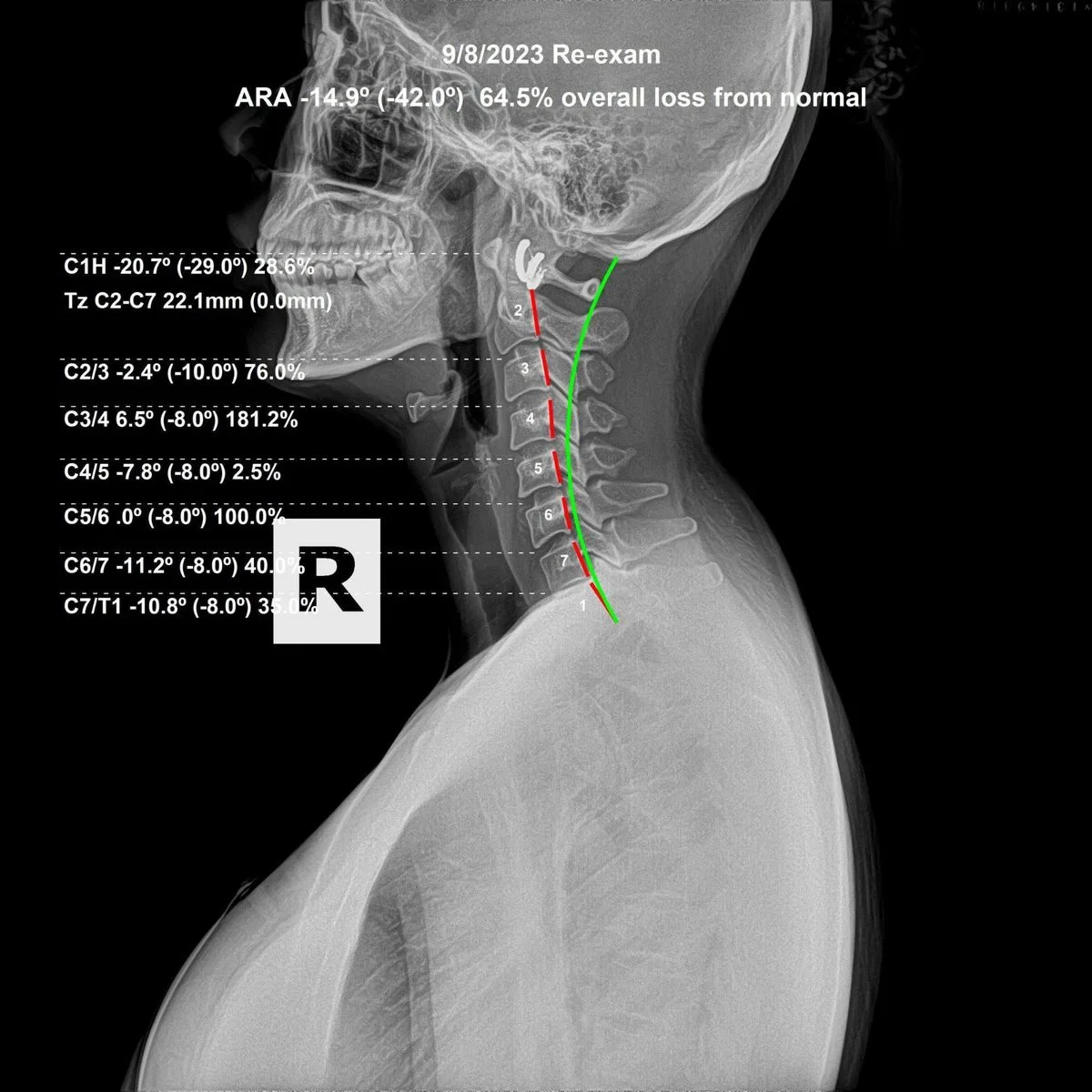
Lateral cervical X-ray. The curve of the neck, vertebral positioning, and disc spaces are all evaluated for subluxation. Dr. Rochet, Royal Palm Beach FL.
I also use leg-length analysis (postural asymmetry from spinal tension) and neurological checks of specific nerve roots. I run these at every visit, not just the first, to decide whether you need an adjustment that day and where.
What it does to your nervous system
Nerve signal interference
Your nervous system runs everything. The brain sends signals down the spinal cord and out through the nerve roots to every organ, muscle, and tissue. When a cervical vertebra subluxates, it puts pressure or tension on the nerve root at that level, and that disrupts the signal in both directions — brain to body and body to brain.
An important distinction: only about 10% of your nerve fibers are sensory, the ones that carry pain. The other 90% are motor and autonomic — running movement, organ function, immune response, and circulation. That is why a cervical subluxation can sit there for years without any neck pain. The interference is happening. Pain is not always the signal.
This is exactly why I do not wait for symptoms. A subluxation at C1 can be affecting brainstem output, blood pressure, and immune coordination — none of which hurt — while you feel perfectly fine. The only way to know is to look, with X-ray and neurological analysis, not symptom reporting.
Atlas subluxation: the most significant level
The brainstem connection
The atlas (C1) is unique. It is the only vertebra with no disc above it; it sits directly under the skull. And it surrounds the brainstem — the part of the nervous system that runs heart rate, breathing, blood pressure, and all of your automatic functions.
A subluxation at the atlas is not the same as one at C5. The neurological consequences of an atlas misalignment are systemic in a way the lower levels are not. That is why upper cervical chiropractic, focused on the atlas and axis, is its own recognized specialty within subluxation-based practice.
I check atlas and axis positioning on every lateral cervical X-ray I take at the first exam. It is one of the first things I look for, and one of the most significant when it is there.
How cervical subluxation is corrected
The specific adjustment
I correct a cervical subluxation with a specific adjustment aimed at the misaligned vertebra. It starts with a precise X-ray analysis to find which vertebrae are subluxated, the direction of the misalignment, and how much structural change is present. Then I deliver the adjustment to that exact level, moving the vertebra back toward where it belongs and taking away the nerve interference it was creating.
This is not a one-visit fix. Your neck has usually been subluxated for months or years before I ever see it. Real structural change takes time and consistent, specific care. I measure progress with follow-up X-rays — not how you say you feel, but measurable movement on film. That is what separates structural correction from general maintenance.
What correction looks like on X-ray
Before and after
Correction is a process, not an event, and we document it with follow-up X-rays after a period of care. The before-and-after films below show what that actually looks like: measurable, visible change in spinal position and the cervical curve.


What you are seeing is a real change in the position of the cervical vertebrae: the curve deepening, the head coming back over the shoulders, the disc spaces evening out. That is what correction produces when the care is specific, consistent, and analyzed at every visit.
It is also why I require X-rays before I start. Without a baseline film, there is no way to know whether your spine is actually changing, or whether the adjustments are doing what they should.
Subluxation vs. disc herniation
They are different conditions
These are not the same thing, though people mix them up constantly. A cervical disc herniation is a structural failure of the disc — the cartilage cushion between vertebrae — where disc material pushes out and can press on a nerve root or the cord directly. It is a mechanical injury.
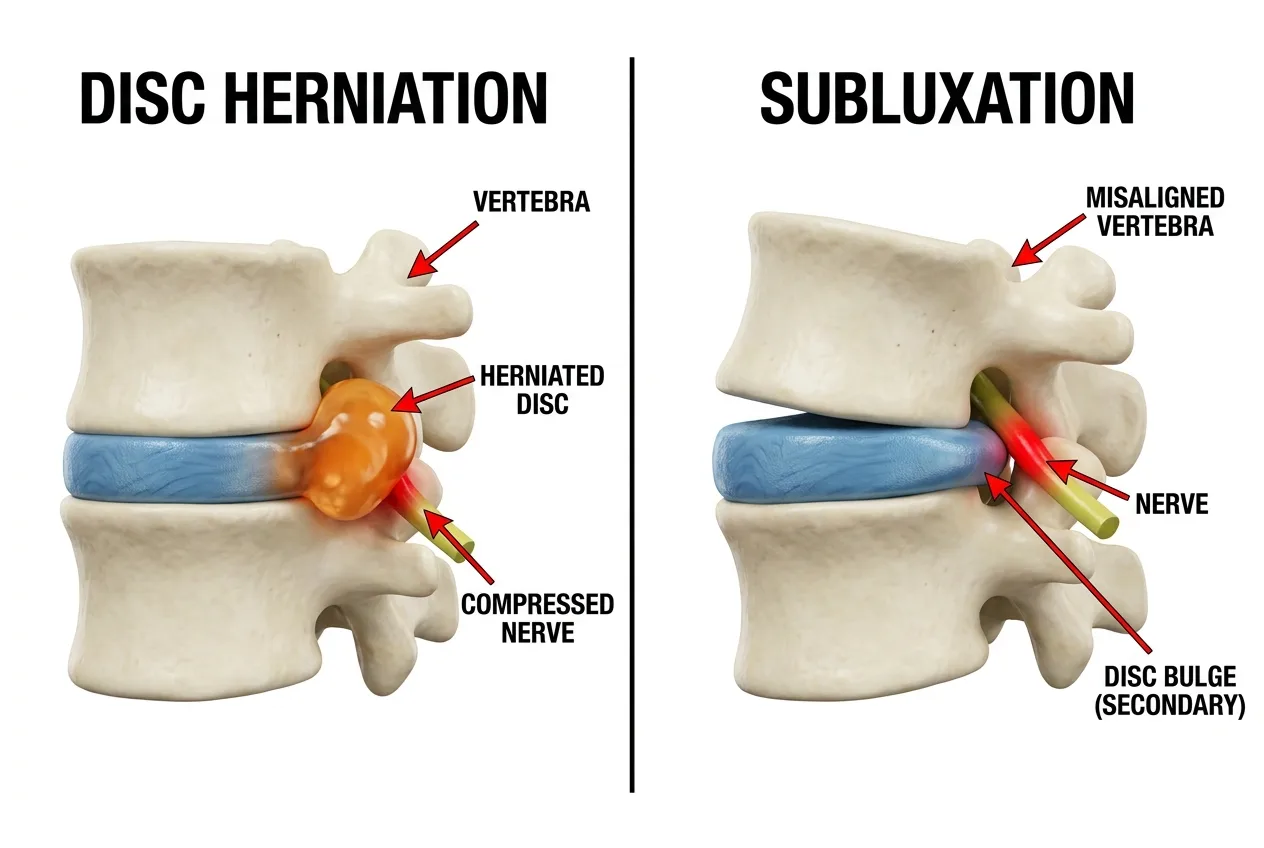
Left: disc herniation — nucleus pulposus ruptures through the annulus and directly compresses the nerve root. Right: subluxation — the vertebra itself is misaligned, creating nerve interference through positional pressure. Different mechanisms, different corrections.
A cervical subluxation is a misalignment of the vertebra itself, creating nerve interference through position and pressure, not necessarily disc material. The two can coexist: chronic subluxation loads the disc abnormally, which speeds up degeneration and makes herniation more likely over time.
I address the vertebral position. In a lot of cases, correcting the subluxation takes the mechanical stress off the disc and lets it recover. Where there is significant herniation with neurological compromise, co-managing with other providers can be the right call.
Who gets cervical subluxation?
Risk and progression
Everyone is susceptible. Your cervical spine takes physical stress from day one; the birth process itself produces measurable forces on the neck. Falls, forward head posture from screens, sports hits, car accidents, and the steady compression of gravity all add up over time.
Côté P, et al. "The burden and determinants of neck pain in workers: results of the Bone and Joint Decade 2000–2010 Task Force on Neck Pain and Its Associated Disorders." Spine. 2008;33(4 Suppl):S60–74. PubMed ↗
It is not a matter of age or how active you are. I have found significant cervical subluxation in adults with no injury history at all who simply accumulated postural stress for decades.
I have found significant cervical subluxation in newborn babies due to the stress of the birth process.
The spine does not fix itself. Subluxations that go uncorrected tend to compound: what starts as a positional misalignment turns, over years, into disc narrowing, curve loss, and degenerative change you can see on film.
Catching it early always beats catching it late. That is the whole argument for having your spine checked periodically, symptoms or not.