What sciatica actually is
Sciatica is a nerve problem, and Harvard Health estimates that as many as 40% of people experience it at some point in their lives. It runs the whole range. For some people it is a mild ache that radiates into the glute and leg. For others it is severe pain and weakness that leaves them bent to one side, unable to stand up straight.
Sciatica is not really a diagnosis of its own. It is a signal, and true sciatica comes from pressure on the lumbar nerve roots where they exit the lower spine — most often a vertebral subluxation at L4, L5, or S1 pressing directly on the nerve root, or a disc herniation that is itself the result of a subluxation nobody corrected. That is different from piriformis syndrome, where the sciatic nerve is irritated lower down by the piriformis muscle deep in the buttock. It gets called sciatica, but it is a separate problem with a different source.

The sciatic nerve
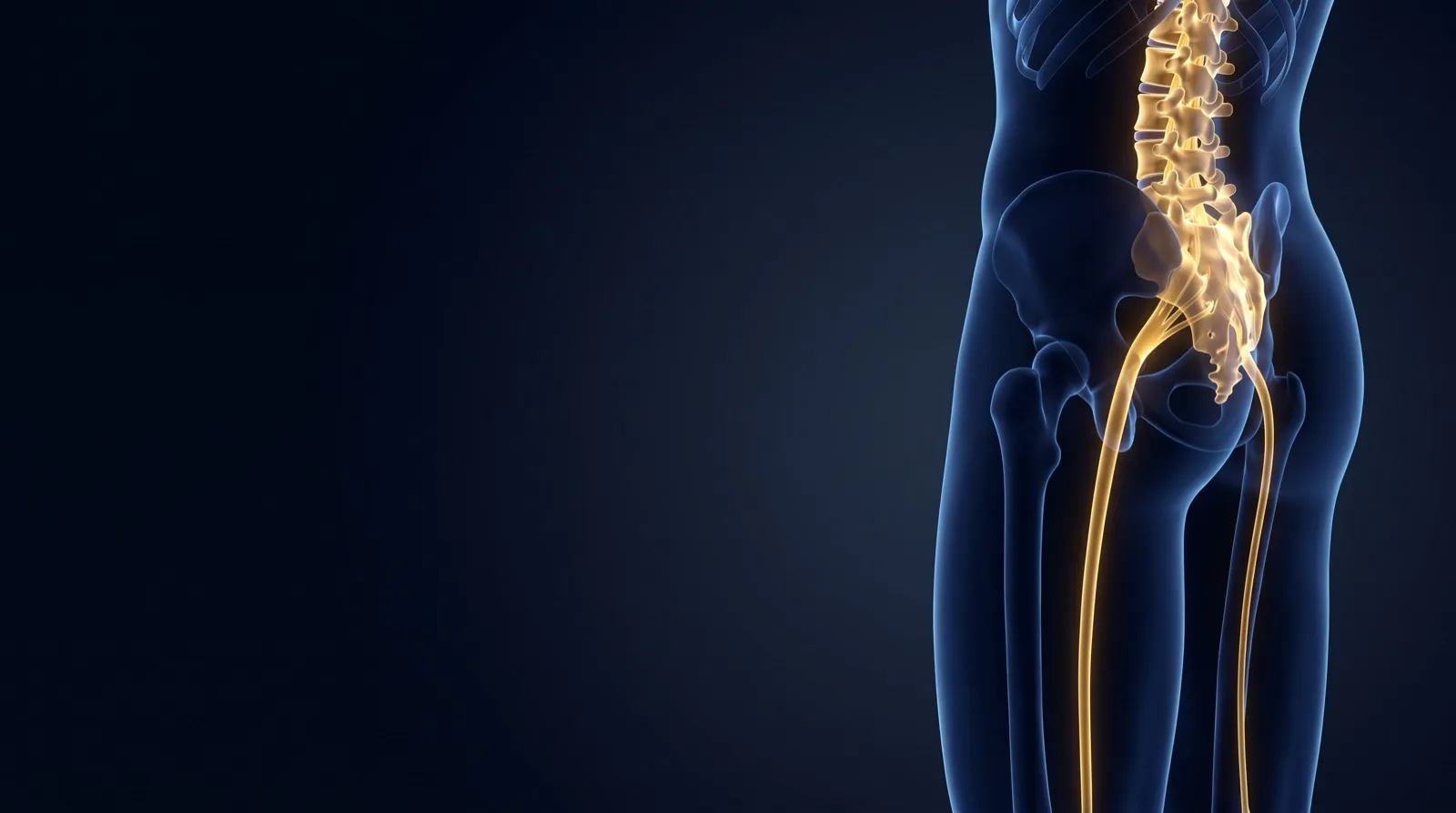
The sciatic nerve is the longest nerve in your body. It starts as separate roots at L4, L5, and S1 in the lower spine, exits on each side, joins together in the pelvis into one thick trunk, passes under the piriformis muscle behind the hip, and runs down the back of the leg, splitting at the knee into branches that carry on to the foot.
That is a long way to travel. When the nerve gets pinched at the root, where it leaves the spine, the whole length downstream feels it. Glute pain, a burning thigh, a cramping calf, numbness in the foot. Those are not four separate problems. They are one nerve, pressed at one spot, telling you about it all the way down.
That is why sciatica can feel like a foot problem or a hip problem when it is neither. The feeling is down the leg. The compression is at the spine. So that is where the correction has to happen — not where it hurts, but where the nerve is actually being pinched.
Sciatica answers to one thing: taking the pressure off the nerve. Not to drugs that quiet the signal the nerve is sending.
Why most sciatica approaches fall short
Anti-inflammatories, steroid injections, pain management. They all turn down the signal the nerve is sending. None of them removes what is pressing on it. As long as the structure stays the same, the compression stays, and the pain comes back the moment the medication wears off.
Surgery can cut away the tissue pressing on the nerve, but if the subluxation that caused the disc or joint to compress it in the first place is never corrected, it tends to come back. And surgery can run up to $150,000 and still leave the structural root untouched.
Subluxation-based correction goes straight at the structural cause: the misaligned vertebra creating the compression. Correct that and the pressure comes off, and the sciatic nerve is free to do its job again.
Correcting the cause
Sciatica usually comes from one of two structural problems, and often both:
A) a subluxated lumbar vertebra pressing on the nerve root as it leaves the spine, or
B) a bulging or herniated lumbar disc compressing that same nerve root.
In chronic cases it is usually the two together. When I correct the subluxated vertebra, I take the hard bone off the soft nerve and start moving the spine back toward where it belongs. As the vertebrae line up again, the uneven stress the subluxation put on the disc eases too, which gives the disc a chance to recover.
When the disc is involved
A herniated disc is not a separate thing from subluxation. Most of the time it is the result of one.
A subluxated vertebra loads the disc unevenly. Under that lopsided pressure, year after year, the disc starts to bulge, then herniate, then break down. The nerve compression that follows is the end of a long structural story, not a sudden accident.
That is why so many people tell me their sciatica came "out of nowhere," after bending to pick something up or sleeping wrong. That moment did not cause it. It was the last straw on a disc that had been wearing down for years under a crooked vertebra.
Correcting the subluxation takes that uneven load off the disc. As the vertebra moves back toward position, the pressure normalizes, and when the herniation has not yet calcified, the disc often regains its integrity over the course of corrective care.
Not every sciatica is the same
The level involved changes everything. A subluxation at L4-L5 refers nerve symptoms to a different place than one at L5-S1, and each calls for its own specific correction. That is why the correction has to be aimed at the level actually compressing the nerve, not simply where the leg happens to hurt.
Every case is different
There is no single sciatica protocol that fits everyone. How much care it takes depends on how long the subluxation has been there and how far the disc has been involved. Recent cases often change quickly. Long-standing compression with degeneration takes longer.
What does not change is the aim: correct what is subluxated, take the pressure off the nerve, and let the timeline follow your spine rather than a template.
Restoring quality of life: the outcomes that matter
One case stays with me. Severe sciatica from years of subluxation, a lot of degeneration, disc involvement. His medical doctors had recommended spinal surgery. He crawled into my office asking if chiropractic could do anything for him.
He was in his 70s, so honestly, expectations for big structural change were modest. We followed subluxation-based adjusting and McKenzie disc protocols. After six months of corrective care:
He was snowboarding again. Playing pickleball. And he had his full 6'4" height back. Not because we treated his sciatica, but because we corrected the subluxations causing it and let his body heal itself.


He came back later with an update: no relapse, no return of the sciatica, still exercising and living an active life. Correcting the subluxation did more than ease his symptoms. It gave him his life back.
Serving Royal Palm Beach, Wellington & nearby
People drive in from Wellington, Loxahatchee, West Palm Beach, and right here in Royal Palm Beach for subluxation-based structural care. If you have been managing sciatica with medication and nobody has corrected the structure, it is worth finding out whether the source of the compression can be addressed directly.
A lot of the people I see have already run the medication gauntlet — NSAIDs, muscle relaxers, steroid injections — without any structural change. Some come in after being told surgery is the next step. The first conversation worth having is whether anyone has actually identified and corrected the specific vertebra driving the nerve compression. Usually no one has. That is where I start.
- Lumbar X-ray analysis included with your new patient consultation
- Specific spinal correction based on your individual X-ray findings
- Progress re-examination to track structural change
- Care grounded in correction, not indefinite symptom management